Anaphylaxis as edema focus in tongue and lip is rare but not exceptional (1% treatment). It does not usually affect airway, in our experience is very rare, and improve administrating corticosteroids. Often it happens at the end of drug infusion or immediately after infusion.
The differential diagnosis of tongue bleeding between digastric muscles should be done but the latter would only be logical if there is a discontinuity or injury in tongue or mucosa.
Bleeding complications as infarct hemorrhagic transformation occurs in over 25% of cases. But only 4-6% are considered symptomatic (worsening of over 4 points in NIHSS scale). Hypertension, infarct established large and age are factors involved in its appearance. Therefore in elderly patients failure to control hypertension drug with more than two types of treatments or having to stop more than once infusion of rtPA for control) may be considered as a scarce benefit and increase the risk of hemorrhagic tranformation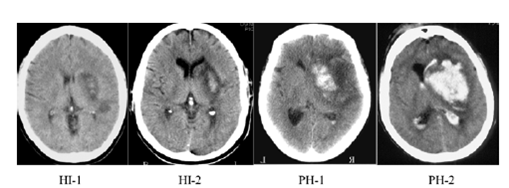 Examples bleeding after rtPA. The PH1-2 are usually symptomatic bleeding (empeormiento> 4 NIHSS points)
Examples bleeding after rtPA. The PH1-2 are usually symptomatic bleeding (empeormiento> 4 NIHSS points)
Other hemorrhagic complications are those that occur after IVT with subgaleals hematomas in these cases it is important to apply pressure over cutaneous haematoma. However a frequent problem is that this can occur with minor bleeding in parenchymal still dangerous rtPA administration.
Neither the present period nor small and easily compressible injuries are contraindications to rtPA.
Small bleeds in the form of epistaxis or hematuria usually associated with the use of sondages that can lacerate the mucous. We recommend not perform urinary sondage l during rtPA infusion.
Another frequent complication are the vasogenic edema often happens after infarct recanalization of large infarcts. Futile recanalization has been associated to this situation just associating a mass effect, being necessary the use of antiedema measures or even early surgery.