The code allows the transfer stroke patient suspected of having a stroke immediately to a hospital with a specialist in neurology able to perform differential diagnosis and where both TAC has a 24h / 365d.
Press here to check Video Cincinnati scale ⇐
Stroke code provides solution to the problem of time in establishing a correct diagnosis of stroke.
His home in our territorial area began in 2005, other territories as Girona pioneered coding three years earlier.
It has managed to increase more than 10% the number of treatments reperfusion stroke pacients all that come to our hospital with suspected stroke, specifically in our center by more than 25%.
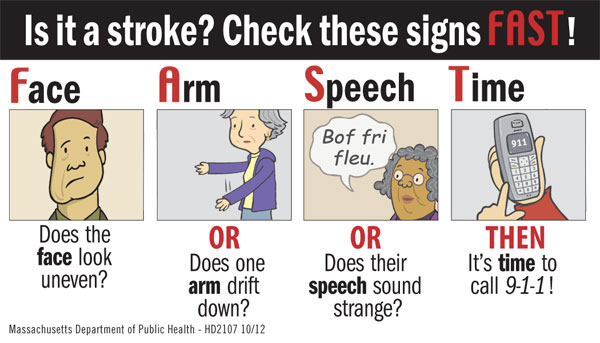
The first part of the activation is to verify that the patient has signs and symptoms consistent with a stroke (either ischemic or hemorrhagic, no semiotic data to differentiate these two subtypes) and proceed activation by SEM, SAMUR, etc. US is set to the FAST acronym in Catalunya RAPID as listed below.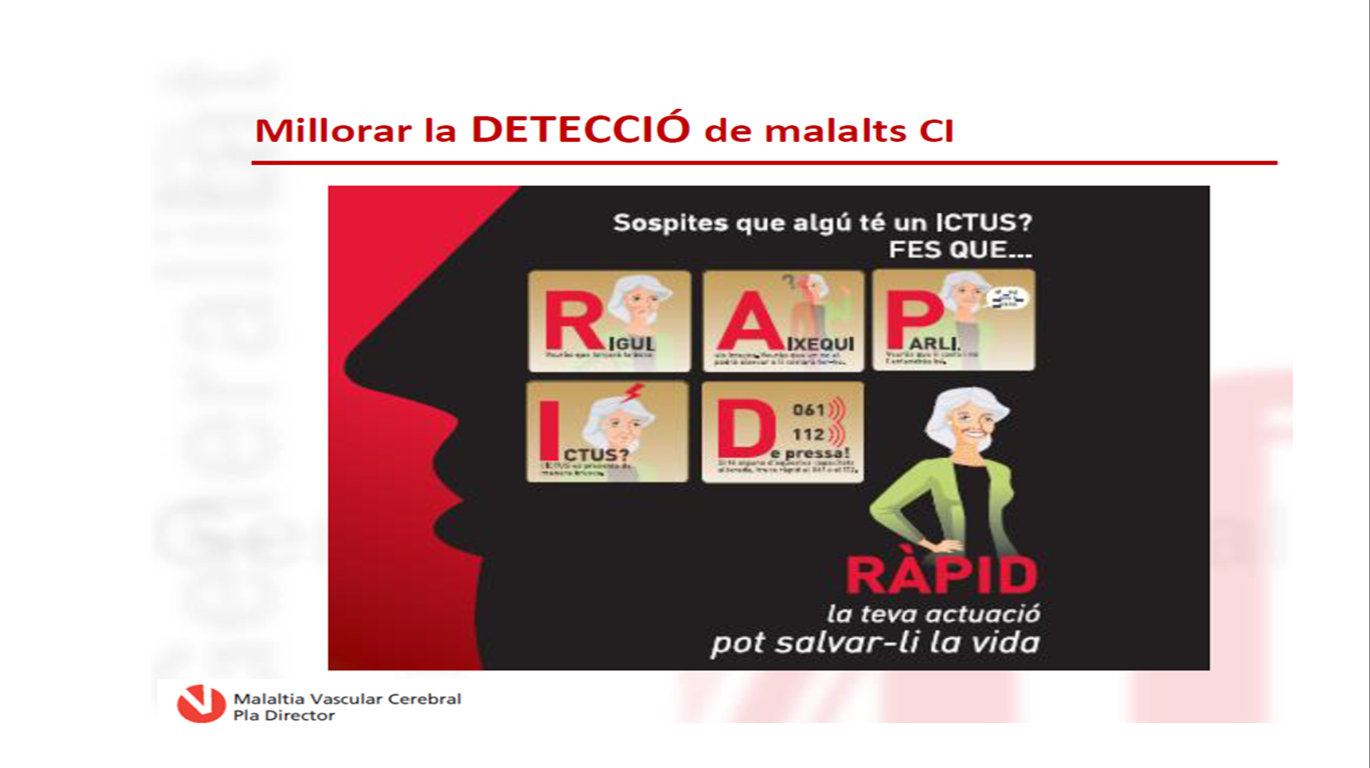
Within a decade the criteria have changed, especially those wide selection groups esaso benefit for reperfusion therapy but experience of professionals is equally effective for diagnosis of stroke whether reperfusion therapy is administered ( age> 80 years, limit> 4.5h start clinical situation with premorbid Rankin could be up to 3 anamnesis (at first it was just up to 0-2 approx.).
This last point is the most critical. Since the course of presenting ischemic stroke (85% of strokes), regardless of age the patient might benefit from some reperfusion therapy (thrombolysis if <4.5h, if occlusion thrombectomy large glass). The only factor that could limit transfer given little benefit in these cases would be an important pre comorbidity, or poor previous functional situation (Rankin scale, difficulty showering, dressing).
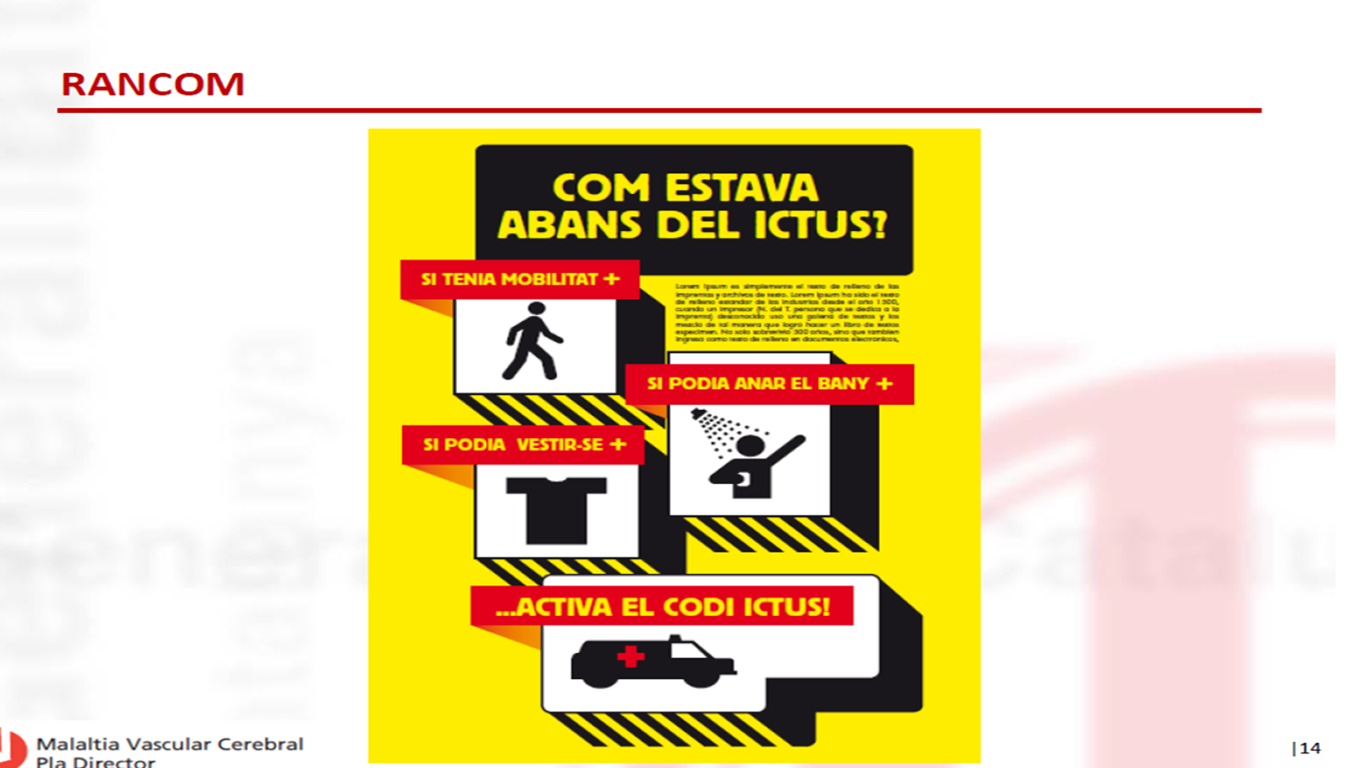
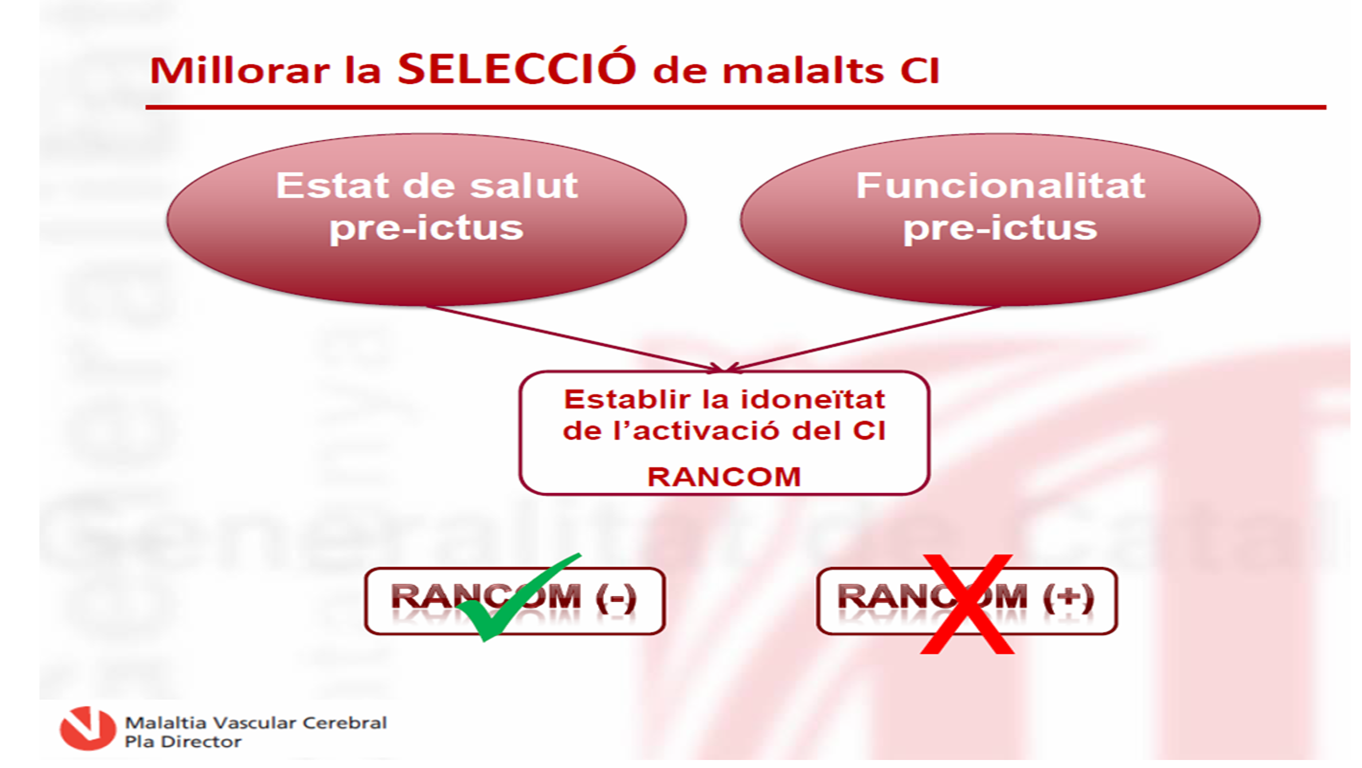
It assesses that if you have a positive RANCOM, stroke code should not be activated, being the strongest criterion for non-activation.

Example: PDMVC. Catalonia Health Department. Criteria STROKE CODE SINCE 2012. (FAST –RAPID, RANCOM – Non Comorbidity, NO LIMIT AGE, WAKE-UP AND UNKNOWUN HOUR ONSET )
Another criterion is the modified start time symptoms (last time the patient was seen well). While start is accepted now limit of 6 hours (in some leaflets to 8am), the stroke of unknown schedule is also acceptable or awakening which could be triggered stroke code because we have multiparameter imaging techniques (CT perufsión) to establish whether there thrombectomy viable tissue if a large vessel occlusion).
Upon recommendation of 2012 different Plans for cerebrovascular disease including Catalonia it states that there is no limit of age provided that previous functionality is good RANCOM – and to be submitted within 8 hours or stroke or even wake vertebrobasilar stroke characteristics > 12 h (given feasibility of this cerebral posterior location). This means that the less in doubt start of the clinic could activate after consultation with specialist successful activation.
Doesn’t matter age, any patient with suspicious stroke symptoms with previous good baseline situation is candidate to activate stroke code.